
-3 2x1.jpg)
The RAIN scale: A good intention that falls short
Radiation protection specialists agree that clear communication of radiation risks remains a vexing challenge that cannot be solved solely by finding new ways to convey technical information.
Earlier this year, an article in Nuclear News described a new radiation risk communication tool, known as the Radiation Index, or, RAIN (“Let it RAIN: A new approach to radiation communication,” NN, Jan. 2025, p. 36). The authors of the article created the RAIN scale to improve radiation risk communication to the general public who are not well-versed in important aspects of radiation exposures, including radiation dose quantities, units, and values; associated health consequences; and the benefits derived from radiation exposures.
* Therapeutic dose for cancer cells. Exposure in normal tissues occurring during a general radiation therapy will be much smaller than these levels.
**Gy is used instead of Sv because the irradiated target is not a human tissue but an object.
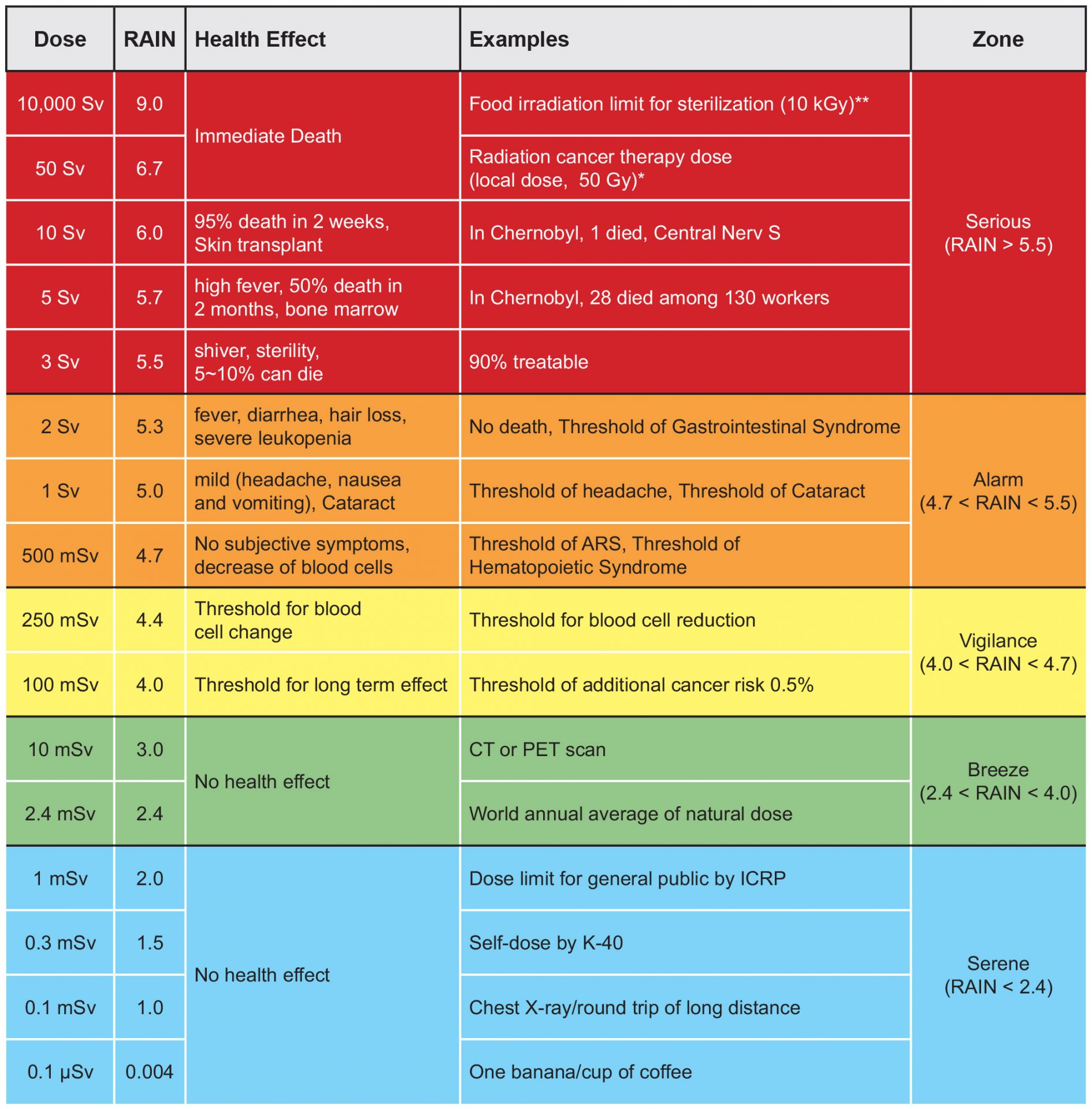
Fig. 1. The RAIN scale. (Source: Jong H. Kim et al., “Let it RAIN: A new approach to radiation communication,” NN, Jan. 2025, p. 36)
Still cloudy
Jong H. Kim, Gyuseong Cho, Kun-Woo Cho, Tae Soon Park, and Keon W. Kang, the RAIN scale creators, modeled their tool off other similar logarithmic scales, such as the International Nuclear and Radiological Event Scale (INES) and the Richter scale for earthquake magnitude characterization.
Unfortunately, logarithmic scales are not readily interpretable by the public. The RAIN scale the authors provided in their article (fig. 1) includes terminology and representations that are prone to public misinterpretation. In the first column, for example, “dose” is not sufficiently explained for the general public. Possible dose quantities include point absorbed dose, point equivalent dose, point dose equivalent, organ equivalent dose, organ dose equivalent, effective dose, and effective dose equivalent.
Furthermore, the unit sievert, used throughout the scale, is not familiar to the public and is defined only for stochastic effects. Organ doses weighted by relative biological effectiveness (RBE), known as the RBE-weighted dose in units of gray-equivalent, should be used to contextualize radiation exposures for tissue reactions (deterministic effects). The scale does not communicate the large variations observed in individual health effects with “dose,” including cancer risk variation (which is impacted by factors such as age and biological sex) and tissue reactions (such as skin erythema and gastrointestinal syndrome).
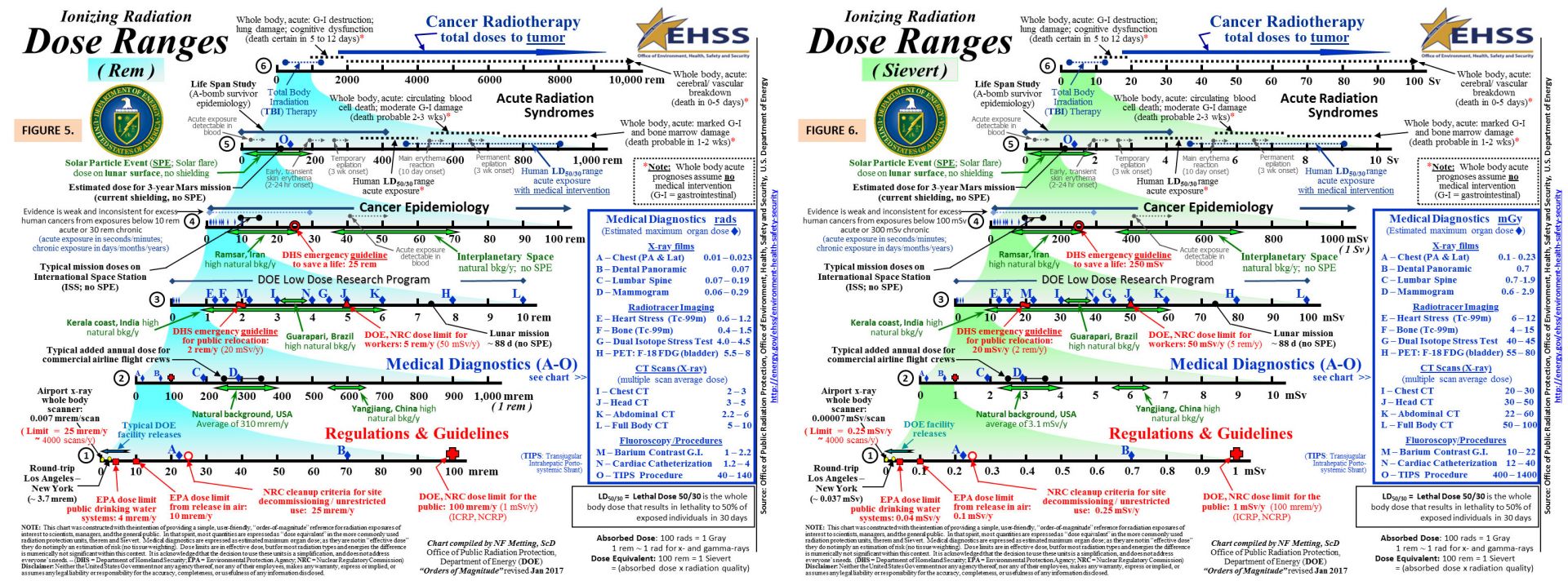
Fig. 2. The DOE-EHSS Ionizing Radiation Dose Ranges chart. (Source: DOE)
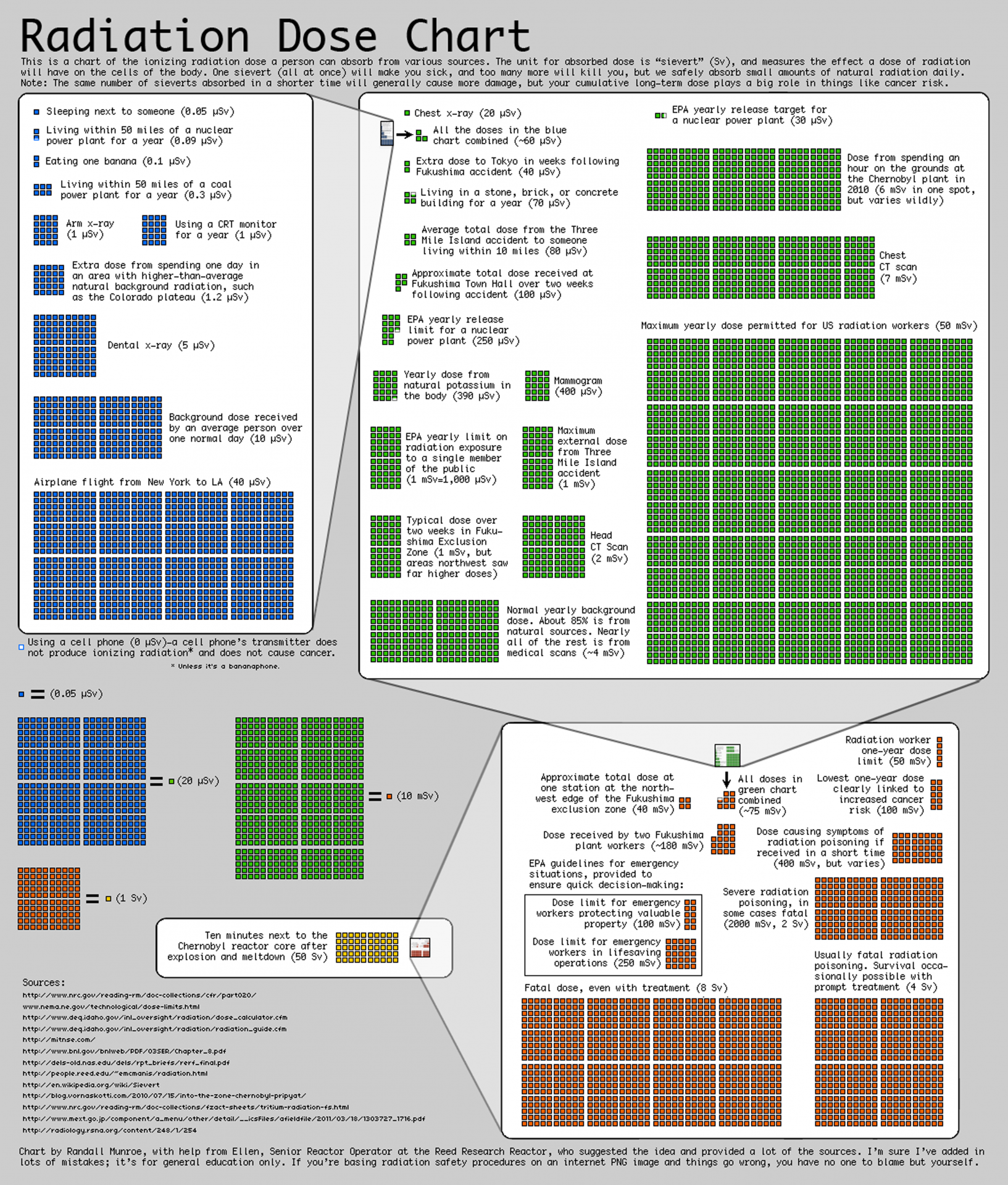
Fig. 3. xkcd radiation dose chart. (Source: Randall Munroe/xkcd)
Finally, to be meaningful to the public, comparisons should be stated in terms of “familiar risks” with similar likelihoods, consequences, and benefits. The RAIN scale instead takes the typical approach of dose comparisons, which in effect compares unfamiliar risks to unfamiliar risks. This tactic is already used by other visual tools, such as the Department of Energy Office of Environment, Health, Safety, and Security (DOE-EHSS) Ionizing Radiation Dose Ranges chart (fig. 2) and the radiation dose chart created by engineer and artist Randall Munroe for his webcomic xkcd (fig. 3).
Breaking down the scale
There are several more specific issues with the RAIN scale. In the following discussion, it is assumed that the exposure to be understood using the RAIN scale is a whole-body uniform photon exposure unless otherwise specified, since each dose quantity essentially has the same numerical value for these conditions (e.g., 1 mGy = 1 mGy-Eq = 1 mSv).
Serene (D < 2.4 mSv). All “serene” exposures are stated to have no health effect, implying that the threshold for any health effect is at least 2.4 mSv. It is true that there are no known tissue reactions that occur at these dose levels. However, as stated in the American Nuclear Society’s Position Statement #41, Risks of Exposure to Low-Level Ionizing Radiation, the true biological relationship between dose and risk of stochastic effects is not well characterized below about 100 mSv, so it is possible that there is some risk—however small—associated with these exposures. The smallest dose presented, 0.1 μSv, is so small as to be essentially meaningless. The banana/cup of coffee comparison has no meaningful relationship with other types of radiation exposures and trivializes the concerns of the public.
Breeze (2.4 mSv < D < 100 mSv). All “breeze” exposures also are stated to have no health effect, implying that the threshold for any health effect is at least 100 mSv. This is misleading for the same reasons stated above for “serene” exposures, although this statement is even more dubious. There is increasing evidence that the true biological relationship between dose and risk of stochastic effects can at least be approximated as linear down to chronic doses of tens of millisieverts. (See, e.g., “The Scientific Basis for the Use of the Linear No-Threshold [LNT] Model at Low Doses and Dose Rates in Radiological Protection,” Journal of Radiological Protection; doi.org/10.1088/1361-6498/acdfd7.)
Additionally, it is at least plausible that a population subject to the world-average natural background exposure could develop cancers that would not be present in a population that is exposed to a much lower background dose. Radon decay products, which almost exclusively dose the lung, account for more than half of the natural background exposure. The lung was assigned a tissue weighting factor of 0.12 by the ICRP (see The 2007 Recommendations of the International Commission on Radiological Protection, ICRP pub. 103). Therefore, the exposed population would be subject to a chronic lung equivalent dose of 10 mSv.
Vigilance (100 mSv < D < 500 mSv). A dose of 100 mSv is explicitly listed as a “threshold for long-term effect.” Virtually all international and national bodies that make radiation protection recommendations advocate for a nonthreshold model for radiation-associated cancer. Paradoxically, the authors have arbitrarily defined a 0.5 percent increase in cancer (mortality) as a “threshold” for stochastic effects, even though smaller increases in cancer mortality risk are possible. This appears to confuse the commonly referenced (and now outdated) threshold of 100 mSv for statistical significance with the rule of thumb of a 5 percent increase in cancer mortality per sievert for general population chronic radiation exposure.
Alarm (500 mSv < D < 3 Sv). The name of this range implies that it is the worst case, even though it is not the most severe “zone” in the RAIN scale. It is not clear what is meant by “subjective symptoms” occurring at the 500 mSv dose level. Furthermore, the threshold for “blood cell change” was previously stated as occurring at 250 mSv, but here a “decrease of blood cells” is referenced. The authors claim a cataract threshold of 1 Sv, even though the most recent ICRP recommendations give 0.5 Gy-Eq as the threshold, with possible thresholds ranging from 0 to 0.8 Gy-Eq.
Serious (D > 3 Sv). The probability of death must be stated in terms of the amount of time between exposure and death (commonly 30 days or 60 days for humans) and whether medical intervention is provided. The lethal dose for 50 percent of the population within 30 days (LD 50/30) is often placed at 4 to 5 Sv or 3.2 to 4.5 Gy. The comparison of 50 Sv with a 50 Gy tumor dose is not meaningful, since cancer radiotherapies are targeted to specific treatment volumes while delivering doses many times smaller to normal tissues. Additionally, the inclusion of a dose of 10,000 Sv lacks biological relevance, as no human has survived exposures resulting in an effective dose approximately 1,000 times smaller than this value.
A recommended path forward
Simply inventing a formula for logarithmic, unitless comparisons is not a panacea for communicating radiation risks with the public. As such, the RAIN scale is not an improvement to existing comparison tools.
The field of radiation protection must move to using tools that help communicate the unfamiliar risks associated with ionizing radiation exposure with those that are familiar to the public in terms of probability, consequences, and benefit. Furthermore, it is crucial that risk communicators avoid stating in conclusive terms that there is no health effect at a given exposure level when one may be present.
Radiation risk communication requires extensive bidirectional conversations to understand public perception and concerns, establish trust, and find ways to properly contextualize risks. The only way forward is to dig in and start having these hard conversations.
Amir A. Bahadori is an associate professor and director of the Radiological Engineering Analysis Laboratory at Kansas State University.